
Territorial inequalities in environmental health
The health status of a population can be affected by a complex set of individual determinants and social and environmental factors. A report by the General Secretary of the Ministries of Social Affairs (SGMAS) and the General Commission for Sustainable Development (CGDD) considered that on a local scale, the issue of environmental and social health inequalities is linked to two compounding elements: the level of the population’s exposure to a degraded living environment and the level of vulnerability to risk factors that can affect health (Besse et al., 2014). Populations experiencing more pronounced precarity would therefore be more exposed to environmental pollution and are more vulnerable to the resulting health effects (WHO, 2012). The French National Health Environment Plans (PNSE1 2004-2008; PNSE2, 2009-2013; PNSE3 2015-2019) prioritize this fight against territorial disparities in terms of environmental and social health inequalities. The PNSE 3 seeks to reinforce this axis by promoting the concept of the exposome, i.e. the cumulative exposure of the population to different physicochemical and biological factors, and by recommending the construction of spatialized indicators (chapter II, actions n ° 34, 39, 41, 42, 52).
Environmental health difficulties: what are the main obstacles?
As defined in the first PNSE, environmental health involves
“all the interactions between humans and their environment and any health effects that are linked to living conditions (exposures in an individual’s private and/or professional life, etc.) and to the contamination of different environments (such as water, air and soil) ”.
This concept of environment is centered around the different living environments of the populations and excludes any possible effects caused by voluntary exposure to pollutants and individual behaviors such as smoking, alcohol consumption or eating habits. The living environment is not limited to the home and outdoor surroundings, but also includes the professional environment. Within the framework of this programme, we are specifically interested in the general population, as defined by the public health code. We consider the environment to essentially be an external living environment (air, water and soil). The latter can also be referred to as a general or natural environment and is governed by the Environmental Code. We therefore exclude occupational exposure, which is governed by legislation for the prevention of occupational risks (Labor Code) and workplace exposures.
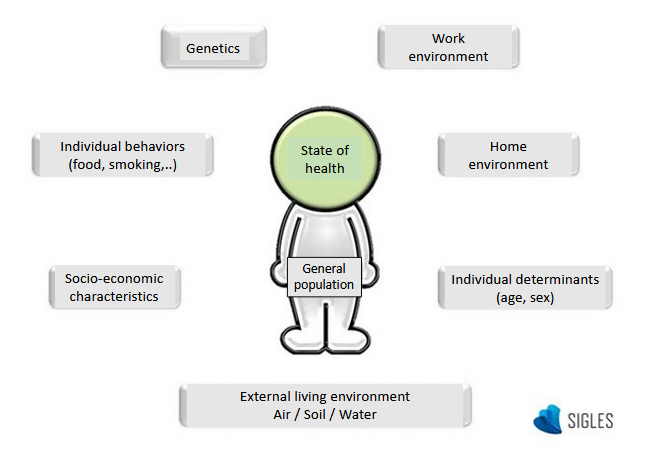
Factors influencing Health.
It has been widely acknowledged for many years now that the quality of the different environmental components, i.e. air, water and soil, can have an impact on health. The World Health Organization (WHO) recently estimated that 23% of premature deaths observed in developed countries in 2012 are attributable to the environment (Prüss-Üstün et al., 2016).
The figures reveal that nearly 3.7 million people (3.4% of deaths) worldwide died prematurely in 2012 due to exposure to outdoor air pollution (WHO, 2014). The decision was made to classify diesel emissions and outdoor air pollution as certain carcinogens in 2013 (WHO, 2015).
Less than 15% (455,000) of these 3.7 million premature deaths are seen in high-income regions. This confirms that socio-economic factors play a key role in health effects, combined with environmental factors.
This report concludes by highlighting the specific link between air pollution and cardiovascular and respiratory diseases, as well as cancers. As such, the European project APHEKOM recently concluded that exceeding the WHO recommendations on atmospheric fine particles (PM2.5) and concluded that levels of atmospheric particles that exceeded recommended WHO values result in 19,000 premature deaths per year in most of the European cities studied, the majority of these deaths being due to cardiovascular causes (Pascal et al., 2013).
However, the multifactorial etiology of environmental diseases and the low specificity of their symptoms make it difficult to characterize this link. In addition, humans are globally exposed to their environment, and they are therefore exposed to all the contaminants that the environment contains. The multiple exposure routes further complicate the identification and determination of environmental risk factors.
In order to better characterize the quality of the living environment of populations, a rapidly expanding national and international regulatory framework has been set up to define and regulate the implementation of environmental monitoring by approved bodies (AASQA) for air monitoring, water boards, and scientific interest groups for soil. This framework is composed of legislation including the 1996 Air and Rational Use of Energy Act (part of the Environment Code), the 2000 Water Framework Directive adapted to local specificities for water development and management plans (‘SDAGE’), and the Soil Framework Directive, which is in the process of being written. Despite this continuous monitoring, our knowledge of environmental quality is still poor in comparison to our knowledge of population health status, mainly due to the cost and difficulty of acquiring data.
All of these findings explain why, with the exception of specific pathologies such as lead poisoning or pleural mesothelioma following exposure to asbestos, few diseases today can be unequivocally attributed to the quality of the environment.
There is a substantial amount of literature describing the link between environmental risk factors and certain pathologies. Air pollution peaks or exposure to a specific air pollutant (Crouse et al., 2012; Katsoulis et al., 2014; Carey et al., 2013) are regularly linked to elevated rates of respiratory and cardiovascular disease. However, few studies consider the role played by background pollution, multiple exposure and environmental quality over the long term.
Little attention has been paid to the possible role played by environmental determinants in other pathologies such as chronic renal failure or inflammatory bowel disease (IBD). Cadmium, for example, could accelerate the process of reaching the final stage of renal failure (Lauwerys et al., 1993; Hellström et al., 2001; Järup et al., 2002). The rapid and large-scale increase observed in the incidence of Crohn’s disease in developed countries since 1950 and the recent appearance of this disease in emerging countries also highlight the role that environmental changes play in pathogenesis (Jantchou et al ., 2006).
There are two approaches that currently seek to answer this need for characterization and confirm a causal link between a pathology and the environment: health risk assessment (HRA) method, which are are based on the source – vector – target continuum (National Research Council, 1983), or epidemiological approaches carried out on an individual scale in patient cohorts or in the general population. Health risk assessments are specific to the site studied, meaning that the results cannot be extrapolated to the general population. Individual epidemiological studies are costly and difficult to implement.
Geographical ecological studies
In this context, geographic (or temporal) ecological studies are a particularly interesting means to explore etiological hypotheses before implementing more interventional studies. Ecological studies aim to detect variations in the occurrence of a disease in space or over time, and relate these variations to environmental and/or social factors. These studies are based on aggregated data (groups of individuals) rather than individual data. This inexpensive and relatively rapid tool can be adapted on a spatial scale, making it ideal for use in public health diagnostics and decision-making (Goria et al., 2011).
These studies do however produce global results that reflect a certain number of biases (Wakefield, 2008), including the ecological bias. The latter includes, for example, the different individual risk factors within the population groups studied. It is therefore difficult to focus on a specific pollutant, since the environmental factors studied cannot be considered to represent the actual exposure of population groups.
In an ecological study, the link between health and the environment is not therefore based on estimating a risk through the exposure of individuals, but is rather achieved by superimposing different types of information and studying whether they evolve separately or together. This information is likely to indicate a link that is characterized by populations with a poor state of health in a degraded environment.
Geographical Information Systems in environmental health
Geographic Information Systems (GIS) are essential tools for the joint study of spatialized parameters relating to the state of the environment, demographic and socio-economic statistics, and population morbidity and mortality rates. These systems can detect environmental, health and socio-economic blackspots (Vine et al., 1997). The additional implementation of spatialized statistical approaches such as geostatistical interpolation methods, disease mapping and spatial cluster detection to these georeferenced indicators provides a solid base of powerful spatialized analysis tools.
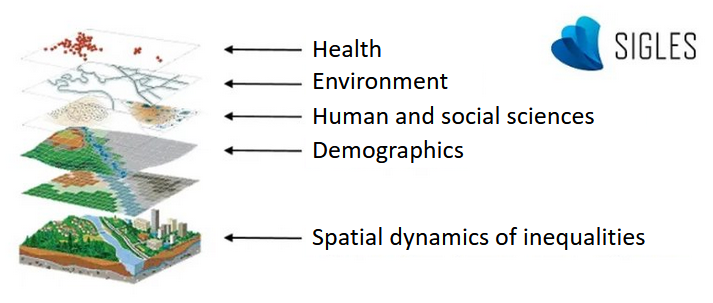
GIS in environmental health (modified, from ESRI France).
A successful spatialized study in environmental health depends not only on the availability of data for a given territory and over an adequate period of time (particularly in terms of the latency time of the health factor studied), but also requires a data format that allows them to be compared. However, environmental, social and health data are very different in nature and type. For institutional reasons of ethics and confidentiality, health indicators (from pathology registers for example) and socio-economic population indicators (taken from the National Institute of Statistics and Economic Studies (Insee) censuses, for example) are calculated and communicated as aggregated data. The information (incidence of illness, value of the precarity indicator, etc.) characterizes a specific population group, which generally corresponds to an administrative unit (county, town, neighborhood, etc.). The majority of data providing information on the quality of environments are geostatistical, and are made up of a sample of georeferenced points which have been assigned a measured indicator such a concentration of pollutant or a biological index. The different formats of these data require the implementation of spatial analysis methods, and this can lead to difficulties when attempting to establish links between the different data.
References
Besse G, Caudeville J, Michelot F, Prisse N, Trugeon A. 2014. Inégalités territoriales, environnementales et sociales de santé. Regards croisés en régions : de l’observation à l’action. SGMAS & CGDD, 68p.
Carey IM, Atkinson RW, Kent AJ, van Staa T, Cook DG, Anderson HR. 2013. Mortality associations with long-term exposure to outdoor air pollution in a national English cohort. Am J Respir Crit Care Med, 187 : 1226-33.
Crouse DL, Peters PA, van Donkelaar A, Goldberg MS, Villeneuve PJ, Brion O, Khan S, Atari DO, Jerrett M, Pope CA, Brauer M, Brook JR, Martin RV, Stieb D, Burnett RT. 2012. Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: a Canadian national-level cohort study. Environ Health Perspect., 120:708-14.
Directive Cadre sur l’Eau. 2000. Directive 2000/60/CE du Parlement européen et du Conseil établissant un cadre pour une politique communautaire dans le domaine de l’eau.
Goria S, Stempfelet M, de Crouy-Chanel P. 2011. Introduction aux méthodes statistiques et aux systèmes d’information géographique en santé environnement – Application aux études écologiques. Saint-Maurice: Institut de veille sanitaire. 65 p. Disponible à partir de l’URL : http://www.invs.sante.fr.
Hellström L, Elinder C-G, Dahlberg B, Lundberg M, Järup L, Persson B, Axelson O. 2001. Cadmium exposure and end-stage renal disease. Am J Kidney Dis, 38: 1001-8.
Jantchou P, Monnet E, Carbonnel F. 2006. Les facteurs d’environnement dans la maladie de Crohn et la rectocolite hémorragique (tabac et appendicectomie exclus). Gastroenterol Clin Biol, 30 : 859-867.
Järup L. 2002. Cadmium overload and toxicity. Nephrol Dial Transplant, 17: 35–9.
Katsoulis M, Dimakopoulou K, Pedeli X, Trichopoulos D, Gryparis A, Trichopoulou A, Katsouyanni K. 2014. Long-term exposure to traffic-related air pollution and cardiovascular health in a Greek cohort study. Sci Total Environ, 490:934-40.
Lauwerys RR, Bernard AM, Buchet J-P, Roels H. 1993. Assessment of the health impact of environmental exposure to cadmium: contribution of the epidemiologic studies carried out in Belgium. Environ Res, 62: 200-6.
Loi sur l’air et l’utilisation rationnelle de l’énergie. 1996. Loi N° 96-1236 du 30 décembre 1996 sur l’air et l’utilisation rationnelle de l’énergie.
National Research Council, Committee on the institutional means for assessment of risks to public health. 1983. Risk assessment in the Federal government: managing the process. National Academy Press Washington, D.C. 191p.
OMS. 2012. Environmental health inequalities in Europe. Copenhagen, OMS Europe. 190p.
OMS. 2014. Burden of disease from the joint effects of Household and Ambient Air Pollution for 2012. Geneva.
OMS. 2015. IARC monographs on the evaluation of carcinogenic risks to humans. Outdoor air pollution. Vol. 109. 454p. Geneva.
Pascal M, Corso M, Chanel O, Declecq C, Badaloni C, Cesaroni G, Henschel S, Maister K, Haluza D, Martin-Olmedo P, Medina S. 2013. Assessing the public health impact of urban air pollution in 25 European cities: results of the Aphekom project. Science of the Total Environment, 449: 390-400.
Prüss-Ustün, A., Wolf, J., Corvalán, C., Bos, R., Neira, M., 2016. Preventing Disease Through Healthy Environments A Global Assessment of the Burden of Disease from Environmental Risks. World Health Organization.
Vine M, Degnan D, Hanchette C. 1997. Geographic Information Systems: Their Use in Environmental Epidemiologic Research. Environmental Health Perspectives, Volume 105, Number 6: 598-605.
Wakefield J. 2008. Ecologic studies revisited. Annual Review of Public Health, 29: 75–90.